Overview

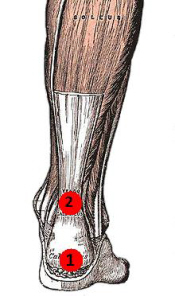
The Achilles tendon is a conjoined tendon composed of the gastrocnemius and soleus muscles with occasional contribution from the plantaris muscle, and it inserts on the calcaneal tuberosity. The plantaris muscle is absent in 6% to 8% of individuals. The Achilles tendon is approximately 15-cm long and is the largest and strongest tendon in the human body. The tendon spirals approximately 90? from its origin to its insertion and this twisting produces an area of stress approximately 2- to 5-cm proximal to its insertion. The tendon has no true synovial sheath; instead it is wrapped in a paratenon. The Achilles tendon experiences the highest loads of any tendon in the body, and bears tensile loads up to 10 times body weight during athletic activities. The tendon most commonly ruptures in a region 2- to 6-cm proximal to its insertion.
Causes
People who commonly fall victim to Achilles rupture or tear include recreational athletes, people of old age, individuals with previous Achilles tendon tears or ruptures, previous tendon injections or quinolone use, extreme changes in training intensity or activity level, and participation in a new activity. Most cases of Achilles tendon rupture are traumatic sports injuries. The average age of patients is 29-40 years with a male-to-female ratio of nearly 20:1. Fluoroquinolone antibiotics, such as ciprofloxacin, and glucocorticoids have been linked with an increased risk of Achilles tendon rupture. Direct steroid injections into the tendon have also been linked to rupture. Quinolone has been associated with Achilles tendinitis and Achilles tendon ruptures for some time. Quinolones are antibacterial agents that act at the level of DNA by inhibiting DNA Gyrase. DNA Gyrase is an enzyme used to unwind double stranded DNA which is essential to DNA Replication. Quinolone is specialized in the fact that it can attack bacterial DNA and prevent them from replicating by this process, and are frequently prescribed to the elderly. Approximately 2% to 6% of all elderly people over the age of 60 who have had Achilles ruptures can be attributed to the use of quinolones.
Symptoms
Tendon strain or tendon inflammation (tendonitis) can occur from tendon injury or overuse and can lead to a rupture. Call your doctor if you have signs of minor tendon problems. Minor tenderness and possible swelling increases with activity. There is usually no specific event causing sudden pain and no obvious gap in the tendon. You can still walk or stand on your toes. Acute calf pain and swelling can indicate a tear or partial tear of the Achilles tendon where it meets the calf muscle. You may still be able to use that foot to walk, but you will need to see a specialist such as an orthopedic surgeon. Surgery is not usually done for partial tears. Sometimes special heel pads or orthotics in your shoes may help. Follow up with your doctor to check for tendonitis or strain before resuming activity, because both can increase the risk of tendon rupture. Any acute injury causing pain, swelling, and difficulty with weight-bearing activities such as standing and walking may indicate you have a tear in your Achilles tendon. Seek prompt medical attention from your doctor or emergency department. Do not delay! Early treatment results in better outcome. If you have any question or uncertainty, get it checked.
Diagnosis
A physician usually can make this diagnosis with a good physical examination and history. X-rays usually are not taken. A simple test of squeezing the calf muscles while lying on your stomach should indicate if the tendon is still connected (the foot should point). This test isolates the connection between the calf muscle and tendon and eliminates other tendons that may still allow weak movement. A word of caution, Achilles tendon rupture is often misdiagnosed as a strain or minor tendon injury. Swelling and the continuing ability to weakly point your toes can confuse the diagnosis. Ultrasound and MRI are tests that can assist in difficult diagnosis. Depending on the degree of injury, these tests can also assist in determining which treatment may be best.
Non Surgical Treatment
As debilitating as they can be, the good news is that minor to moderate Achilles tendon injuries should heal on their own. You just need to give them time. To speed the healing, you can try the following. Rest your leg. Avoid putting weight on your leg as best you can. You may need crutches. Ice your leg. To reduce pain and swelling, ice your injury for 20 to 30 minutes, every three to four hours for two to three days, or until the pain is gone. Compress your leg. Use an elastic bandage around the lower leg and ankle to keep down swelling. Elevate your leg. Prop you leg up on a pillow when you're sitting or lying down. Take anti-inflammatory painkillers. Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen (Advil, Motrin) and naproxen (Aleve) will help with pain and swelling. However, these drugs have side effects, such as an increased risk of bleeding and ulcers. They should be used only occasionally unless your health care provider says otherwise and should be taken with food. Check with your doctor before taking these if you have any allergies, medical problems or take any other medication. Use a heel lift. Your health care provider may recommend that you wear an insert in your shoe while you recover. It will help protect your Achilles tendon from further stretching. Practice stretching and strengthening exercises as recommended by your health care provider. Usually, these techniques will do the trick. But in severe cases of Achilles tendon injury, you may need a cast for six to 10 weeks or even surgery to repair the tendon or remove excess tissue.
Surgical Treatment
In general, for complete tear of the tendon, surgery is recommended. For partial tears, nonsurgical treatment is recommended. However, the selection of treatment depends on the patient, age, level of activity, and other risk factors. Surgery for Achilles tendon rupture is now routine and well established. Surgery is generally suggested for the young, healthy and active individuals. For athletes, surgery is often the first choice of treatment. The Achilles tendon can be repaired surgically by either a closed or open technique. With the open technique, an incision is made to allow for better visualization and approximation of the tendon. With the closed technique, the surgeon makes several small skin incisions through which the tendon is repaired. Irrespective of type of treatment, a short leg cast (plaster) is applied on the operated ankle after completion of the procedure. The advantages of a surgical approach includes a decreased risk of re-rupture rate (0%-5%) the majority of individuals can return to their original sporting activities (within a short time), and most regain their strength and endurance. Disadvantages of a surgical approach include hospital admission, wound complications (for example, skin sloughing, infection, sinus tract formation, sural nerve injury), higher costs, and hospital admission.
The Achilles tendon is a conjoined tendon composed of the gastrocnemius and soleus muscles with occasional contribution from the plantaris muscle, and it inserts on the calcaneal tuberosity. The plantaris muscle is absent in 6% to 8% of individuals. The Achilles tendon is approximately 15-cm long and is the largest and strongest tendon in the human body. The tendon spirals approximately 90? from its origin to its insertion and this twisting produces an area of stress approximately 2- to 5-cm proximal to its insertion. The tendon has no true synovial sheath; instead it is wrapped in a paratenon. The Achilles tendon experiences the highest loads of any tendon in the body, and bears tensile loads up to 10 times body weight during athletic activities. The tendon most commonly ruptures in a region 2- to 6-cm proximal to its insertion.
Causes
People who commonly fall victim to Achilles rupture or tear include recreational athletes, people of old age, individuals with previous Achilles tendon tears or ruptures, previous tendon injections or quinolone use, extreme changes in training intensity or activity level, and participation in a new activity. Most cases of Achilles tendon rupture are traumatic sports injuries. The average age of patients is 29-40 years with a male-to-female ratio of nearly 20:1. Fluoroquinolone antibiotics, such as ciprofloxacin, and glucocorticoids have been linked with an increased risk of Achilles tendon rupture. Direct steroid injections into the tendon have also been linked to rupture. Quinolone has been associated with Achilles tendinitis and Achilles tendon ruptures for some time. Quinolones are antibacterial agents that act at the level of DNA by inhibiting DNA Gyrase. DNA Gyrase is an enzyme used to unwind double stranded DNA which is essential to DNA Replication. Quinolone is specialized in the fact that it can attack bacterial DNA and prevent them from replicating by this process, and are frequently prescribed to the elderly. Approximately 2% to 6% of all elderly people over the age of 60 who have had Achilles ruptures can be attributed to the use of quinolones.
Symptoms
Tendon strain or tendon inflammation (tendonitis) can occur from tendon injury or overuse and can lead to a rupture. Call your doctor if you have signs of minor tendon problems. Minor tenderness and possible swelling increases with activity. There is usually no specific event causing sudden pain and no obvious gap in the tendon. You can still walk or stand on your toes. Acute calf pain and swelling can indicate a tear or partial tear of the Achilles tendon where it meets the calf muscle. You may still be able to use that foot to walk, but you will need to see a specialist such as an orthopedic surgeon. Surgery is not usually done for partial tears. Sometimes special heel pads or orthotics in your shoes may help. Follow up with your doctor to check for tendonitis or strain before resuming activity, because both can increase the risk of tendon rupture. Any acute injury causing pain, swelling, and difficulty with weight-bearing activities such as standing and walking may indicate you have a tear in your Achilles tendon. Seek prompt medical attention from your doctor or emergency department. Do not delay! Early treatment results in better outcome. If you have any question or uncertainty, get it checked.
Diagnosis
A physician usually can make this diagnosis with a good physical examination and history. X-rays usually are not taken. A simple test of squeezing the calf muscles while lying on your stomach should indicate if the tendon is still connected (the foot should point). This test isolates the connection between the calf muscle and tendon and eliminates other tendons that may still allow weak movement. A word of caution, Achilles tendon rupture is often misdiagnosed as a strain or minor tendon injury. Swelling and the continuing ability to weakly point your toes can confuse the diagnosis. Ultrasound and MRI are tests that can assist in difficult diagnosis. Depending on the degree of injury, these tests can also assist in determining which treatment may be best.
Non Surgical Treatment
As debilitating as they can be, the good news is that minor to moderate Achilles tendon injuries should heal on their own. You just need to give them time. To speed the healing, you can try the following. Rest your leg. Avoid putting weight on your leg as best you can. You may need crutches. Ice your leg. To reduce pain and swelling, ice your injury for 20 to 30 minutes, every three to four hours for two to three days, or until the pain is gone. Compress your leg. Use an elastic bandage around the lower leg and ankle to keep down swelling. Elevate your leg. Prop you leg up on a pillow when you're sitting or lying down. Take anti-inflammatory painkillers. Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen (Advil, Motrin) and naproxen (Aleve) will help with pain and swelling. However, these drugs have side effects, such as an increased risk of bleeding and ulcers. They should be used only occasionally unless your health care provider says otherwise and should be taken with food. Check with your doctor before taking these if you have any allergies, medical problems or take any other medication. Use a heel lift. Your health care provider may recommend that you wear an insert in your shoe while you recover. It will help protect your Achilles tendon from further stretching. Practice stretching and strengthening exercises as recommended by your health care provider. Usually, these techniques will do the trick. But in severe cases of Achilles tendon injury, you may need a cast for six to 10 weeks or even surgery to repair the tendon or remove excess tissue.
Surgical Treatment
In general, for complete tear of the tendon, surgery is recommended. For partial tears, nonsurgical treatment is recommended. However, the selection of treatment depends on the patient, age, level of activity, and other risk factors. Surgery for Achilles tendon rupture is now routine and well established. Surgery is generally suggested for the young, healthy and active individuals. For athletes, surgery is often the first choice of treatment. The Achilles tendon can be repaired surgically by either a closed or open technique. With the open technique, an incision is made to allow for better visualization and approximation of the tendon. With the closed technique, the surgeon makes several small skin incisions through which the tendon is repaired. Irrespective of type of treatment, a short leg cast (plaster) is applied on the operated ankle after completion of the procedure. The advantages of a surgical approach includes a decreased risk of re-rupture rate (0%-5%) the majority of individuals can return to their original sporting activities (within a short time), and most regain their strength and endurance. Disadvantages of a surgical approach include hospital admission, wound complications (for example, skin sloughing, infection, sinus tract formation, sural nerve injury), higher costs, and hospital admission.
 RSS Feed
RSS Feed
