Overview

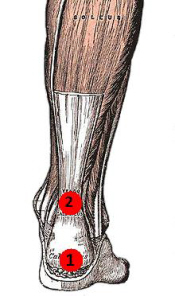
The Achilles' tendon is located in the leg just behind and above the heel. As the connection between the heel and calf muscle, its function is to allow the bending of the foot downwards. Generally if there is a tear to the Achilles' tendon it will be known as a rupture. This can be a partial tear or a complete tear, although partial tears are much rarer.
Causes
As with any muscle or tendon in the body, the Achilles tendon can be torn if there is a high force or stress on it. This can happen with activities which involve a forceful push off with the foot, for example, in football, running, basketball, diving, and tennis. The push off movement uses a strong contraction of the calf muscles which can stress the Achilles tendon too much. The Achilles tendon can also be damaged by injuries such as falls, if the foot is suddenly forced into an upward-pointing position, this movement stretches the tendon. Another possible injury is a deep cut at the back of the ankle, which might go into the tendon. Sometimes the Achilles tendon is weak, making it more prone to rupture. Factors that weaken the Achilles tendon are as follows. Corticosteroid medication (such as prednisolone) - mainly if it is used as long-term treatment rather than a short course. Corticosteroid injection near the Achilles tendon. Certain rare medical conditions, such as Cushing's syndrome, where the body makes too much of its own corticosteroid hormones. Increasing age. Tendonitis (inflammation) of the Achilles tendon. Other medical conditions which can make the tendon more prone to rupture; for example, rheumatoid arthritis, gout and systemic lupus erythematosus (SLE), lupus. Certain antibiotic medicines may slightly increase the risk of having an Achilles tendon rupture. These are the quinolone antibiotics such as ciprofloxacin and ofloxacin. The risk of having an Achilles tendon rupture with these antibiotics is actually very low, and mainly applies if you are also taking corticosteroid medication or are over the age of about 60.
Symptoms
You may notice the symptoms come on suddenly during a sporting activity or injury. You might hear a snap or feel a sudden sharp pain when the tendon is torn. The sharp pain usually settles quickly, although there may be some aching at the back of the lower leg. After the injury, the usual symptoms are a flat-footed type of walk. You can walk and bear weight, but cannot push off the ground properly on the side where the tendon is ruptured. Inability to stand on tiptoe. If the tendon is completely torn, you may feel a gap just above the back of the heel. However, if there is bruising then the swelling may disguise the gap. If you suspect an Achilles tendon rupture, it is best to see a doctor urgently, because the tendon heals better if treated sooner rather than later. A person with a ruptured Achilles tendon may experience one or more of the following. Sudden pain (which feels like a kick or a stab) in the back of the ankle or calf, often subsiding into a dull ache. A popping or snapping sensation. Swelling on the back of the leg between the heel and the calf. Difficulty walking (especially upstairs or uphill) and difficulty rising up on the toes.
Diagnosis
Your doctor diagnoses the rupture based on symptoms, history of the injury and physical examination. Your doctor will gently squeeze the calf muscles, if the Achilles tendon is intact, there will be flexion movement of the foot, if it is ruptured, there will be no movement observed.
Non Surgical Treatment
Nonsurgical treatment involves extended casting, special braces, orthotics, and physical therapy. Avoids the normal complications and expenses of surgery. Some studies show the outcome is similar to surgery in regard to strength and function. There is risk of an over-lengthened tendon with inadequate tension. Extended immobilization can lead to more muscle weakness. Nonsurgical treatment has a higher incidence of re-rupture than surgical repair. Nonsurgical treatment is often used for nonathletes or for those with a general low level of physical activity who would not benefit from surgery. The elderly and those with complicating medical conditions should also consider conservative nonsurgical treatment.

Surgical Treatment
This injury is often treated surgically. Surgical care adds the risks of surgery, there are for you to view. After the surgery, the cast and aftercare is typically as follows. A below-knee cast (from just below the knee to the tips of the toes) is applied. The initial cast may be applied with your foot positioned in a downward direction to allow the ends of the tendon to lie closer together for initial healing. You may be brought back in 2-3 week intervals until the foot can be positioned at 90 degrees to the leg in the cast. The first 6 weeks in the cast are typically non-weight bearing with crutches or other suitable device to assist with the non-weight bearing requirement. After 6 weeks in the non-removable cast, a removable walking cast is started. The removable walking cast can be removed for therapy, sleeping and bathing. The period in the removable walking cast may need to last for an additional 2-6 weeks. Your doctor will review a home physical therapy program with you (more on this program later) that will typically start not long after your non-removable cast is removed. Your doctor may also refer you for formal physical therapy appointments. Typically, weight bearing exercise activities are kept restricted for at least 4 months or more. Swimming or stationary cycling activities may be allowed sooner. Complete healing may take 12 months or more.
The Achilles' tendon is located in the leg just behind and above the heel. As the connection between the heel and calf muscle, its function is to allow the bending of the foot downwards. Generally if there is a tear to the Achilles' tendon it will be known as a rupture. This can be a partial tear or a complete tear, although partial tears are much rarer.
Causes
As with any muscle or tendon in the body, the Achilles tendon can be torn if there is a high force or stress on it. This can happen with activities which involve a forceful push off with the foot, for example, in football, running, basketball, diving, and tennis. The push off movement uses a strong contraction of the calf muscles which can stress the Achilles tendon too much. The Achilles tendon can also be damaged by injuries such as falls, if the foot is suddenly forced into an upward-pointing position, this movement stretches the tendon. Another possible injury is a deep cut at the back of the ankle, which might go into the tendon. Sometimes the Achilles tendon is weak, making it more prone to rupture. Factors that weaken the Achilles tendon are as follows. Corticosteroid medication (such as prednisolone) - mainly if it is used as long-term treatment rather than a short course. Corticosteroid injection near the Achilles tendon. Certain rare medical conditions, such as Cushing's syndrome, where the body makes too much of its own corticosteroid hormones. Increasing age. Tendonitis (inflammation) of the Achilles tendon. Other medical conditions which can make the tendon more prone to rupture; for example, rheumatoid arthritis, gout and systemic lupus erythematosus (SLE), lupus. Certain antibiotic medicines may slightly increase the risk of having an Achilles tendon rupture. These are the quinolone antibiotics such as ciprofloxacin and ofloxacin. The risk of having an Achilles tendon rupture with these antibiotics is actually very low, and mainly applies if you are also taking corticosteroid medication or are over the age of about 60.
Symptoms
You may notice the symptoms come on suddenly during a sporting activity or injury. You might hear a snap or feel a sudden sharp pain when the tendon is torn. The sharp pain usually settles quickly, although there may be some aching at the back of the lower leg. After the injury, the usual symptoms are a flat-footed type of walk. You can walk and bear weight, but cannot push off the ground properly on the side where the tendon is ruptured. Inability to stand on tiptoe. If the tendon is completely torn, you may feel a gap just above the back of the heel. However, if there is bruising then the swelling may disguise the gap. If you suspect an Achilles tendon rupture, it is best to see a doctor urgently, because the tendon heals better if treated sooner rather than later. A person with a ruptured Achilles tendon may experience one or more of the following. Sudden pain (which feels like a kick or a stab) in the back of the ankle or calf, often subsiding into a dull ache. A popping or snapping sensation. Swelling on the back of the leg between the heel and the calf. Difficulty walking (especially upstairs or uphill) and difficulty rising up on the toes.
Diagnosis
Your doctor diagnoses the rupture based on symptoms, history of the injury and physical examination. Your doctor will gently squeeze the calf muscles, if the Achilles tendon is intact, there will be flexion movement of the foot, if it is ruptured, there will be no movement observed.
Non Surgical Treatment
Nonsurgical treatment involves extended casting, special braces, orthotics, and physical therapy. Avoids the normal complications and expenses of surgery. Some studies show the outcome is similar to surgery in regard to strength and function. There is risk of an over-lengthened tendon with inadequate tension. Extended immobilization can lead to more muscle weakness. Nonsurgical treatment has a higher incidence of re-rupture than surgical repair. Nonsurgical treatment is often used for nonathletes or for those with a general low level of physical activity who would not benefit from surgery. The elderly and those with complicating medical conditions should also consider conservative nonsurgical treatment.
Surgical Treatment
This injury is often treated surgically. Surgical care adds the risks of surgery, there are for you to view. After the surgery, the cast and aftercare is typically as follows. A below-knee cast (from just below the knee to the tips of the toes) is applied. The initial cast may be applied with your foot positioned in a downward direction to allow the ends of the tendon to lie closer together for initial healing. You may be brought back in 2-3 week intervals until the foot can be positioned at 90 degrees to the leg in the cast. The first 6 weeks in the cast are typically non-weight bearing with crutches or other suitable device to assist with the non-weight bearing requirement. After 6 weeks in the non-removable cast, a removable walking cast is started. The removable walking cast can be removed for therapy, sleeping and bathing. The period in the removable walking cast may need to last for an additional 2-6 weeks. Your doctor will review a home physical therapy program with you (more on this program later) that will typically start not long after your non-removable cast is removed. Your doctor may also refer you for formal physical therapy appointments. Typically, weight bearing exercise activities are kept restricted for at least 4 months or more. Swimming or stationary cycling activities may be allowed sooner. Complete healing may take 12 months or more.



 RSS Feed
RSS Feed
